As you can see, there are many causes of high cholesterol, and dietary cholesterol and dietary saturated fats are leading causes of high cholesterol. The dietary cholesterol and saturated fat causes of high cholesterol can be taken care of by following our sample diet for lowering high cholesterol, and by also using out cholesterol diet planner - both are diets to lower cholesterol. |
Contents:
|
Obviously, if there is an illness or chemical etc that is causing one or more of the five organs to produce too much cholesterol, then that will need to be medically diagnosed and rectified, to stop it being a cause of high cholesterol.
The rest of this article is focused primarily on understanding the inter-relationship of obesity and inactivity (lack of physical exercise) as the primary cause of high cholesterol in the industrialized world. However, the rest of "What causes high cholesterol?" does become somehwat technical, and you may need to come back several times to fully grasp it.
Cholesterol abnormalities lead to death and disability of millions each year, as high cholesterol is a cause of heart disease, cardiovascular disease and stroke.
Because of this public health problem, the regulation of cholesterol in the body is a topic of vigorous research. In fact, cholesterol metabolism is the most decorated Nobel Prize topic in Physiology or Medicine.
Scientists have determined how cholesterol is absorbed from the diet, how it is metabolized, and excreted.
Doctors have identified various reasons that we need cholesterol in the body and found that our bodies must synthesize cholesterol if we do not consume enough of it in our diet.
Medical science has also determined in great detail how certain forms of cholesterol and related molecules work to cause disease in the blood vessels. From this information, drugs have been created to alter this system and improve cardiovascular health, which has saved countless lives and reduced the incidence of heart attack and stroke.
Despite an enormous amount of research on various aspects of cholesterol metabolism, there is an embarrassing lack of information regarding the way that our own actions affect cholesterol metabolism.
Perhaps you are thinking: We know that obesity leads to heart disease and cholesterol is the link, isn’t that enough?
Well, it is not that simple.
Large numbers of scientific studies are based on associations. They take a group of similar people and follow them over time and see who develops disease and who does not. Then scientists state that there is an association between obesity and heart disease.
We know that obese people develop heart disease, diabetes, and certain other diseases more often than slender people.
Also, it has been shown that those people that exercise regularly have fewer diseases than those that do not, on average.
What is not as clear is what happens to cholesterol regulation at the cellular and molecular level during obesity and inactivity.
While doctors can prescribe a number of drugs to alter cholesterol metabolism and prevent disease, only very recently have scientists begun to focus on the direct impact of obesity, inactivity, unhealthy diet, and other behaviors and their direct role in disrupting cholesterol regulation.
Our body has a rather complex way of regulating how it processes fat and cholesterol in the body, liver, and blood. There are mechanisms that govern absorption of cholesterol from the gut, ways in which the liver processes that cholesterol, even ways in which proteins in the blood handle various forms of cholesterol and fat.
On average, we eat between 200 and 500 mg of cholesterol from various sources each day. Another 1,000 mg of cholesterol is released into the gut daily when the liver and gallbladder release bile into the gastrointestinal tract. We evacuate quite a bit of cholesterol in our feces each day as well, so our body cholesterol levels are changing all of the time.
In order for cholesterol to perform its many tasks in the body, like forming the backbone for hormone molecules or adding flexibility to cell membranes, humans must eat or synthesize about 900 mg of cholesterol per day.
Primarily the liver processes, packages, and excretes this cholesterol for the rest of the body.
What should be striking about this cholesterol bookkeeping is that humans secrete more cholesterol from the body and liver into the GI system than we eat on a daily basis.
Therefore, even if one ate half as much cholesterol each day, the overall amount of cholesterol formed would only be decreased by about 10 percent.
If one eats less cholesterol, the liver manufactures more of it. Likewise, if one eats more cholesterol, the liver scales back synthesis.
While other tissues are capable of synthesizing cholesterol besides the liver, the liver is the main organ for blood cholesterol regulation, especially LDL (bad cholesterol).
Because cholesterol-laden foods are foods that also carry fats that can drive cholesterol metabolism. Fats, depending on their type and degree of saturation, can lead shift cholesterol processing toward LDL or HDL formation. Also, the cholesterol in our diets can adversely affect cholesterol metabolism over time, if we are consuming too much of it.
The old adage that oil (or fat) and water don’t mix is true. In order for fats to be processed in a human body (which is mostly water), cholesterol and fat must be packaged into globules that are soluble in water. By now, most of us have heard of LDL (low density lipoproteins), HDL (high density lipoproteins), and triglycerides—the cholesterol that physicians measure in the blood in order to diagnose disease. But cholesterol can exist as various particles like chylomicrons, chylomicron remnants, VLDL (very low density lipoproteins), LDL, and HDL, among others. These different forms of cholesterol are defined by their relative size as well as their relative composition of fats, proteins and cholesterol. For our purposes, they can be thought of as floating blobs.
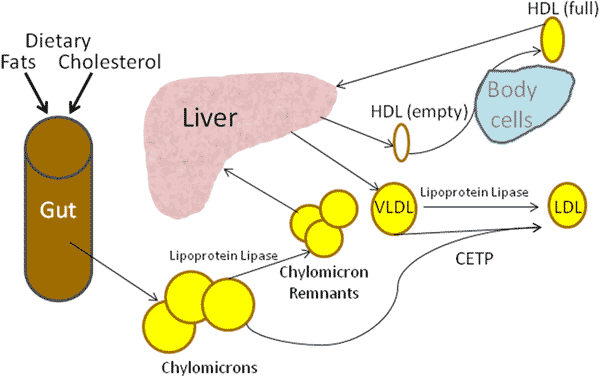
The fats that we eat are dissolved by bile salts (think soap for the GI tract) and form chylomicrons.
These chylomicrons are absorbed across the small intestine, into the lymphatic system, and later enter the blood stream through the thoracic duct.
Once in the blood stream, chylomicrons are processed by an enzyme found in the wall of the blood vessels, and on the cell membranes of fat and muscle cells called lipoprotein lipase.
Lipoprotein lipase removes some of the triglycerides from a chylomicron to form a chylomicron remnant. The liver absorbs these chylomicron remnants and processes them into VLDL particles and empty HDL particles.
VLDL cholesterol particles are converted into LDL by lipoprotein lipase or a protein called CETP. CETP can also directly convert chylomicrons into LDL and vice versa.
The empty HDL particles take cholesterol and lipids from the tissues to become mature HDL particles.
While LDL and VLDL lead to arterial disease, HDL is digested harmlessly. This removal of fat and cholesterol from tissues for degradation by the liver is one of the reasons that HDL is also known as good cholesterol. HDL particles carry cholesterol in a healthy direction, so to speak.
All of this is quite complex but understanding how cholesterol is normally regulated has allowed scientists to then understand how cholesterol regulation is altered by certain states, such as obesity and inactivity.
For example, lipoprotein lipase is an enzyme that is important in regulating triglyceride levels, processing chylomicrons, and overall cholesterol metabolism.
Lower amounts of lipoprotein lipase activity tend to shift cholesterol metabolism toward lower HDL levels and affects how triglycerides are processed the body. Reducing HDL effectively alters the cholesterol ratio in a bad way, which can result in having too much LDL (bad) cholesterol present in the blood - effectively you have caused high cholesterol.
Animal experiments in which levels of lipoprotein lipase are increased show a tendency towards less diet-induced atherosclerosis and dyslipidemia.
If scientists genetically construct animals that have high levels lipoprotein lipase in muscle, they can prevent the animals from becoming obese. Apparently the energy from fats (lipids) are used as energy rather than being stored as adipose tissue (fat cells).
Alternatively, if scientists genetically construct animals that have low levels of lipoprotein lipase in adipose tissue (fat cells), they can prevent obesity in animals that are allowed to overeat.
The same thing takes place in humans, though of course, they are not genetically altered by scientists!
When people are sedentary, the activity of lipoprotein lipase selectively increases in fat cells, more than muscle cells. Thus triglycerides are diverted to storage in fat cell rather than being used as energy in muscle cells.
If you are clever, you may think to yourself: why don’t they make a drug that blocks lipoprotein lipase in fat cells or make a medicine that increases the amount of the protein in muscle cells.
On the face of it, this could be a treatment for obesity. Unfortunately, shunting triglycerides towards muscle can cause its own problems. When triglycerides and fatty acid metabolites accumulate in muscle, it can lead to insulin resistance. Insulin resistance is the primary problem in type 2 diabetes mellitus.
Regular, moderately strenuous exercise can increase the amount of lipoprotein lipase activity in skeletal muscle. This is one of the ways in which exercise, even over the short term, can improve cholesterol metabolism. Increased lipoprotein lipase activity on muscle cell membranes shunts triglycerides into muscle.
However, since the body is exercising and the muscles require energy, the fatty acids and triglycerides are not accumulating, but are being expended as energy. In this way insulin resistance does not occur since triglycerides are being taken from the blood for use, not storage.
Conversely, skeletal muscle atrophy or deterioration causes lipoprotein lipase levels in muscle to decrease. This is a problem for several reasons.
Either lipoprotein lipase activity is on a continuum, vigorous exercise on one end and complete inactivity on the other, or each state has opposing effects on the body. There is some evidence that the latter is true.
When a body is inactive, red oxidative muscle fibers have a 10 fold lower lipoprotein lipase activity.
However, when a body undergoes regular exercise, white glycolytic fibers enjoy an increase in lipoprotein lipase activity of 2.5 times.
In fact the body synthesizes new lipoprotein lipase enzymes in response to exercise but there does not seem to be a “shutting off” of this synthetic machinery during inactivity (breaks in activity).
What does seem to occur is that the body actively suppresses lipoprotein lipase expression (production) after periods of inactivity - when the person appears to no longer be exercising anymore.
The reason for these exercise-dependant changes is not known; however, it does provide a mechanistic link between exercise and cholesterol metabolism.
Exercising or not exercising leads to changes in cholesterol metabolism in our muscles at the molecular level. Exercising can help counteract the causes of high cholesterol.
Most people agree with the following statement: If I do not exercise, I will get fat which will cause my cholesterol to become high.
In many people, all of these things occur; inactivity occurs along with obesity, increased LDL levels, and decreased HDL levels. Again, though, the causative link is not always clear. Certainly there are obese people that get regular exercise. Likewise, people that regularly exercise die of heart disease and people with normal weight have terrible cholesterol levels. For these reasons scientists wish to understand the mechanisms that underlie obesity and cholesterol metabolism, ultimately to better help patients.
Adipose tissue tends to absorb as many triglycerides and fatty acids as it possibly can. Fat cells make proteins that shuttle fat from the bloodstream into fat cells. The more fat cells there are, the more of this protein that is around. In many ways it can be thought of as a snowball effect: fat cells beget more and bigger fat cells.
The adipocyte or fat cell was historically considered like an attic or closet for the body's energy stores; put extra calories into them when we don't need them, pull them out when we do.
However, the adipocyte is now being recognized as a metabolically active cell and one that produces a number of cytokines, hormones, and other proteins. We do know that visceral obesity (obesity in deep layers around the abdomen) is strongly associated with high triglycerides and low HDL, the molecular reasons for this and its regulation are less clear.
The general theory is that more fat cells (of the visceral type) release factors and produce proteins that shift cholesterol balance toward the high trigs, low HDL direction, which very much predisposes one to suffering from high cholesterol. Unfortunately that is the state-of-the-art, and as much as we know at this time.
Alternatively, muscles that are active create more muscle cells along with new lipoprotein lipase molecules on muscle cells. In slender people with decent lean muscle mass, the balance of lipoprotein lipase is tipped in favor of muscle versus fat.
There is still much left to be learned about cholesterol metabolism in both the normal and diseased states.
New medications are being developed that target various molecular regulation points in the system.
Even the existing cholesterol medications can shift cholesterol metabolism in favor of health. These medicines can be extremely helpful, even life-saving.
Short of medications, though, exercise and avoiding obesity naturally achieve the things that scientists are struggling to accomplish in the lab: more lean muscle and less adipose tissue which leads to healthy lipoprotein lipase levels and its beneficial effects on cholesterol metabolism.
Charlton-Menys, V., & Durrington, P. (2007). Human cholesterol metabolism and therapeutic molecules. Exp Physiol , 93 (1), 27-42.
Dietschy, J., Turley, S., & Spady, D. (1993). Role of liver in the maintenance of cholesterol and low density lipoprotein homeostasis in different animal species, including humans. J Lipid Res , 34 (10), 1637-59.
Hamilton, M., Hamilton, D., & TW, Z. (2007). Role of Low Energy Expenditure and Sitting in Obesity, Metabolic Syndrome, Type 2 Diabetes, and Cardiovascular Disease. Diabetes , 56, 2655-67.
Hamilton, M., Hamilton, D., & Zderic, T. (2004). Exercise physiology versus inactivity physiology: an essential concept for understanding lipoprotein lipase regulation. Exerc Sport Sci Rev , 32, 161–6.
KJ, W. (2008). Molecular processes that handle — and mishandle — dietary lipids. J Clin Invest , 118 (10), 3247–59.
Written by Michael T. Sapko M.D., Ph.D., and edited by Donald Urquhart.